
It refers to the most common type of premature fusion of a cranial suture, which leads to varying degrees of frontal bossing as well as occipital coning.
The term Craniosynostosis describes the premature fusing of the joints between the bone plates in the skull of an infant. That results in specific patterns of abnormal skull growth.
Some people define this condition as a congenital deformity that can get divided into several types determined by the affected structure and the pattern of the growth.
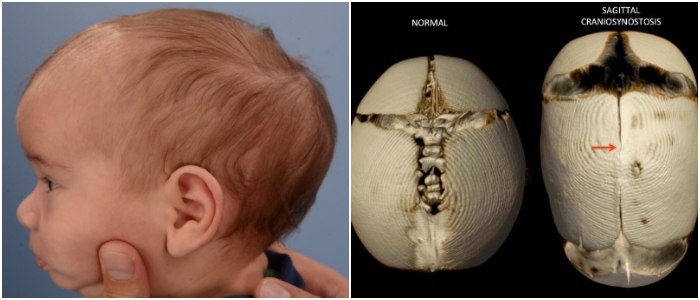
One of the most common types is Sagittal Craniosynostosis. As its name suggests, this condition affects the sagittal suture that runs from the front to the back at the top of the head.
Sagittal Craniosynostosis results in the head of the infant growing longer and narrower than the usual and healthy pattern.
Half of the cases of premature skull closure are patients with Sagittal Craniosynostosis.
Causes
Medical experts are not sure as to what is the specific factor that leads to the development of Sagittal Craniosynostosis.
Some suggest a possible genetic basis to the condition due to the fact it seems to get passed on from parent to child in a small number of families.
Those who support this particular theory are still looking for the gene that could potentially cause Sagittal Craniosynostosis in infants.
Other doctors believe that the cause of this abnormal skull growth is the position of the baby in the womb, which could probably alter the shape of the head.
Regardless of the cause, the result is the same in nearly all cases. The premature fusion of the sagittal suture forces the skull bones to grow at the coronal and lambdoid sutures.
Signs and Symptoms
Sagittal Craniosynostosis features a bony ridge over the prematurely fused sagittal suture, which an expert can either see or feel.
The head becomes elongated in the anterior-posterior diameter and remarkably shortened in the biparietal diameter.
The fontanelle, an anatomical feature that consists of soft membranous gaps or sutures where frontal and parietal bones meet, is either absent or closed.
The skull will look noticeably long when viewed from the side and from above. The head will likely be a lot wider near the forehead while getting narrower towards the back.
When looking straight on at the infant’s face, the forehead will look more prominent, while the sides of the skull look narrow.
Aside from the physical aspects of the condition, Sagittal Craniosynostosis may raise intracranial pressure, which can lead to other issues such as speech and language delay.
Such sings may appear between the ages of three and five years. That is why some kids with Sagittal Craniosynostosis will likely need help from a language therapist to make up for such developmental issues.
However, these particular symptoms don’t occur in all cases as several children with this condition don’t display speech impairment or any similar symptoms.
Sagittal Craniosynostosis Diagnosis
More often than not, medical experts don’t need specific diagnostic tests to confirm if a kid has Sagittal Craniosynostosis.
The characteristic appearance of the affected skull, in other words, the deformity of the head is often enough to diagnose this condition.
However, some may suggest tests such as X-rays, Magnetic Resonance Imaging (MRI), or Computed Tomography (CT) scans to monitor the skull bones growth during any potential treatment.
Even when some doctors acknowledge genetic factor as a potential cause of Sagittal Craniosynostosis, genetic testing is not useful in making a diagnosis because the genes responsible are still unknown.
Treatment
The typical way to deal with this condition is through surgical correction.
However, cases of Sagittal Craniosynostosis may require a multidisciplinary team approach consisting of craniofacial surgeons, neuro (brain) surgeons, ophthalmologists, as well as other specialists.
The best moment to operate an infant is within the first months of life.
Usually, the treatment involves re-opening the fused suture and widening the skull by opening up the coronal and the lambdoid sutures on both sides of the head.
But, the methods and techniques used may vary depending on the severity of the child’s condition or the age of the patient.
More often than not, these procedures lead to significant improvement in the skull’s shape, and the vast majority of the patients grow up to lead healthy lives.



